Short summary: I had an emergency appendectomy on Saturday 18 March 2023, after being taken to hospital by ambulance late the day before. This post is a compilation of notes, emails, and Facebook posts I wrote at the time and in the days following, plus my memory of what happened.
Friday 17 March 2023
There’s always time for new experiences! Today I had an ambulance ride to hospital and tomorrow I get my appendix removed!
Around 2pm I had some abdominal cramping and thought it was my guts/wind. At 3.30pm I went to pee and had bad pain in my lower right side when getting up from my office chair, and even worse pain when trying to get up from the toilet. It was a sharp pain like I’ve never felt before, and a pain I certainly couldn’t ignore—this was not going away, it was getting worse. I asked my dear husband (DH) to confirm where my appendix is (he knows far more about anatomy than me). Yep, the appendix was right where I was having pain and I knew I’d never had mine out. He offered to take me to the doctor, but that could be 2 week wait! I said I’d call the ambulance. He said he could take me but I refused because an ambulance will do an initial assessment, give drugs for the pain, let the hospital know I’m coming and what their initial assessment is, and admit me to emergency via a different route. If he took me, we could be in triage with the general public for hours before getting seen.
I called the ambulance just after 4pm, and, based on where we live, I knew it would be 30 minutes at least before it got to me. I stood for the entire time while I was waiting as sitting or moving was excruciatingly painful. The ambulance arrived around 5pm (from the Brunswick Junction subcentre) and the volunteer ambos (the angels called Rodney and Wendy) did an initial assessment, measured my blood sugar and blood pressure, asked me lots of questions, took lots of notes on their iPad, and gave me the ‘green whistle‘ (a device that dispenses a pain inhibitor straight to the brain), then rolled me into the ambulance on their fancy collapsible gurney and I was at Bunbury Regional Hospital’s emergency department by 6pm (no sirens and no fast speed, thank goodness). Fortunately, ours was the only ambulance in the ambulance bay (BONUS: no ramping at 6pm on a Friday!) and I was the only one in the triage area at the ambulance entrance, which meant it didn’t take long for the handover to the hospital (into a wheelchair) and they could depart for other calls. At home I’d told my DH NOT to come in until I called once I knew what was going on—there was nothing he could do, and until we knew what it was and how long I might be in hospital (if at all), there was just no point.

Despite an easy entry into the hospital, and then past the main triage area to the ‘fast track’ area, much of the rest of the night was spent waiting (and sucking on the green whistle). I estimate it was about an hour before I saw a doctor (Dr Rachel), who drew blood, put in an IV line, prodded and poked around my belly (she was very gentle), got me to pee in a tiny container** then set me to wait in another area. After more waiting, I was taken further into the hospital to wait some more, this time for a CT scan. The operator told me he’d inject a dye into my IV line and that it would feel like I wanted to pee (yep!), but that was the drug/dye marker. I had to hold my arms over my head (while lying on the narrow platform), which is not something I found easy (2 shoulder surgeries will do that). After several trips in and out of the CT scanner, I was left outside to wait in my wheelchair (not one I could propel myself) for someone to collect me and take me back to the previous waiting area. I asked the operator what the dye did and he explained that it goes into the blood and quickly goes to all areas of the body. If there are areas of infection/inflammation, the dye will concentrate there because the blood is trying to fight the nasties. If the dye was really obvious at my appendix, then that would confirm my initial self-diagnosis. (BTW, the ambulance people had said that while it may be appendix, it could also be something like kidney stones or a twisted bowel or something else entirely.)
The nurses then put me on a drip for pain and hydration (but I wasn’t able to have any food in case they needed to operate that night—not that I felt hungry!) while they waited for the results of all my tests (the CT scans had to be checked by people in Perth—thank goodness for the internet!). Around 10:30pm a nurse came out and told me it looked like it was my appendix, but that would be confirmed soon by a doctor. Around 11pm or later, the emergency surgeon (Dr Natasha) sat with me to explain what would happen next and to get my consent, and to ask many of the same questions I’d already been asked numerous times since I made that call to 000 some 7 hours before (I know they have to do this to cover their asses, but really?? When you’re in pain and drugged up and can’t think clearly, this is the last thing you want). The scan had confirmed the appendix hadn’t burst, which they likely knew because I didn’t have the symptoms of a burst appendix. And I was told they’d do surgery tomorrow to remove the appendix (likely laparoscopic surgery, with 3 small incisions, though she warned me that in about 10% of cases they have to cut you open). She also said that I would have to curtail my activities for at least a week, possibly two or more—rest and Netflix were to be my priorities, no cooking or cleaning, no lifting anything (possibility of a hernia), no driving for 1-2 weeks (an emergency braking situation could also cause a hernia), etc.
Somewhere in there I called my DH and asked him to bring a bag of stuff in for me (I’d phoned him throughout the night as I’d found out various things, so while he was worried, I don’t think he was panicking as I was keeping him up-to-date). Oh, and someone brought me a very welcome sandwich (I hadn’t eaten for 12+ hours by then and could have it prior to surgery in the morning as it was outside the fasting times). My DH arrived around midnight and soon after I was taken to a bed on the day surgery ward. The nurse quickly shooed him out (I think he got lost getting out of the hospital and ended up in the private hospital next door and exited via their front doors!) and asked me to have a pre-op shower with a special soap, got me prepped with drugs, IV drip (delivering painkillers too), oxygen prongs, ear plugs, and a compression socks to combat DVT etc. I think she did an ECG as well.
The operation is scheduled for first thing in the morning. I tried to sleep but even in the middle of night, hospitals are noisy places with all the different beeps of the various machines—the ear plugs certainly helped, but I was limited in how much I could move, what with the pain (masked) and the various bits and piece sticking out of me.
** About tiny urine collection containers… Really? 50% of the population is female and those collection bottles just don’t suit the female anatomy, especially when you’re in excruciating pain if you move. It’s 2023 yet we women still have to suffer the indignity of peeing over ourselves while trying to position a tiny container underneath ourselves to try to get a urine sample into the container. They want mid-stream? They’re lucky they get ANYTHING! Challenge to inventors: Devise a urine collection container for female anatomy.
Saturday 18 March 2023
Next morning I was told I was first on the surgical list and that the operation would happen around 8am. One of those doing the surgical rounds about 7am was Dr Natasha from the night before, which was comforting. From what she said, I was under the impression she’d be doing my surgery.
By 9am nothing had happened. I was still in bed waiting. And the reason was that the scheduled anaesthetist had called in sick because his 2 kids had gastro and he didn’t want to give it to anybody else. The hospital had to call in an emergency anaesthetist but he wasn’t due until after 10:30am (it’s a regional town so there aren’t many around—with those times, it’s possible he had to come from Busselton, Mandurah or even Perth). Eventually, I was wheeled into theatre at 11:00am, so my surgery (and everyone else’s that day) was pushed back for 3 hours. Which means Dr Natasha didn’t perform my surgery, even if she’d been scheduled to, because her shift would’ve ended by then.
One thing I recall before I went into surgery is that they put sticky things on my forehead (as well as around my heart). I was told the ones on my forehead were to measure my brain activity—normal is 100% and when it drops to 30% with the anaesthetic, I’d be well under and they can start the surgery.
Of course, I have no memory of the surgery at all, just being wheeled into the operating theatre and squirming painfully onto the table from my bed, trying not to get any of the IV lines etc. caught up. Then nothing.
I recall people talking to me as I was coming to, but I couldn’t respond with anything intelligible, so I held my thumbs up to let them know I was hearing them and responding. By 3:45pm I was fully awake and in the day surgery ward, though in a different bay. There was lots of post op monitoring by the nurses for the first 6 hours, and a huge number of different beeps. And painkillers into the IV line. And a visit from my DH.
I slept well—lots of drugs in my system plus ear plugs. No pain… and no appendix either!

Sunday 19 March 2023
All clear to go home this morning, with strict instructions from the nurses and doctors about what I can and can’t do, which includes no cooking! My DH is so pleased….. Not! 😁
Basic rules are rest and Netflix! Have emailed my clients that I’m not available all this coming week and possibly the following week, and why.
Moving very gingerly and carefully, mouth tastes like crap no matter how many times I clean my teeth (drugs?), showering is interesting as the dressings, which I can’t see, have to be changed (DH has been wonderful). I’m taking all the drugs (including antibiotics) but not the heavy painkillers—just Panadol and Nurofen as advised. Can’t use the foot thingy on my recliner as it was super hard to push in with my legs before the operation and would no doubt rip things apart inside if I tried now, so I’m sitting fairly upright in the chair and using a footstool for my feet (new powered recliners are in our future?). Getting into and out of the car is done super carefully. For the first few days post-hospital I slept at least 3 hours in the afternoon, in addition to normal sleep at night—I never do that, so obviously my body needs that extra sleep to heal.
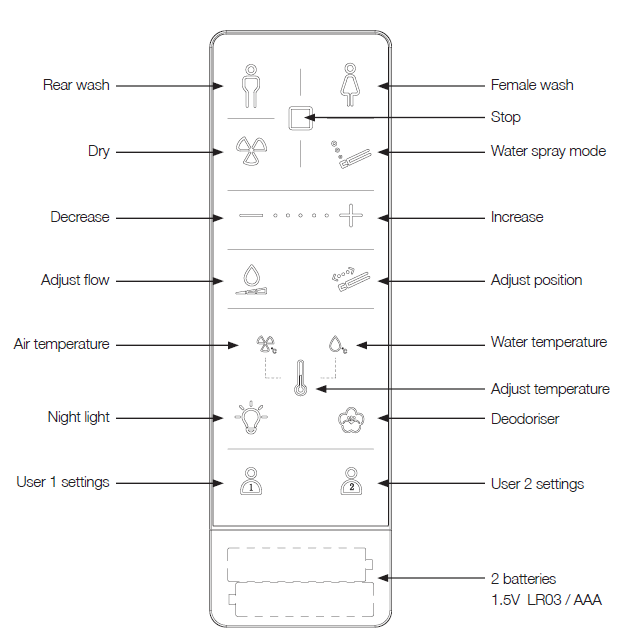
And I’ve given thanks for the smart toilet and grab rails that were only installed a couple of weeks ago as part of our en suite bathroom reno! The grab rail certainly came in useful the first few days, as did the toilet’s in-built bidet function, which meant I didn’t have to twist my body to wipe (yeah, TMI!) and thus put my healing body in danger of herniating. Another reason for getting a bidet I hadn’t thought of…
Days since
Each day the pain has been abating, and what I can do gets a little easier. To get me out of the lounge chair, DH took me to see my parents on Tuesday, and we went for another drive on Wednesday too, stopping for a lovely lunch overlooking the Dawesville Cut near Mandurah. By Thursday I could sit at my computer for a short time, and by Friday 24 March the horrible taste had all but gone (thank goodness—it was very metallic and put me off eating or drinking anything other than water), and I could spend more time in my office chair. Sitting at the dining table is still a bit sore, because I’m bent forward to read the newspaper, do the crosswords etc.
Silver lining
I had a realisation that all this was incredibly well-timed (you’ve got to look for a silver lining, right?). The conference I’ve been attending and speaking at in the US since 2015 (except COVID years) started this week (23 March) in Columbus, Ohio. Some 6 months ago, which is usually about when I book airfares, accommodation etc. and make plans for visiting friends and family or doing a course, I decided that I was still COVID-shy and still wasn’t ready to get on a plane. Besides, the airfares to the US were horrendously high in all classes, AND Qantas still owed me several thousand dollars, which I’d been trying to get from them since August 2022 (they eventually paid up earlier this month). So I decided not to go this year’s conference. Which was bloody lucky for me!
Had I decided to go, I either would’ve already been in the US when this happened, OR somewhere in the many flights between Western Australia and Ohio, one of which is about 17 hours non-stop. I cannot IMAGINE what either of those scenarios would’ve been like. Neither would have had good outcomes. Having appendicitis on a long flight across the Pacific would likely have meant either dealing with the pain with whatever the flight crew (or a doctor) had on board and hoping my appendix hadn’t burst or that bursting wasn’t imminent, or causing the plane to detour to a Pacific island to get medical attention for me, and thus likely being offloaded somewhere from where I would find it hard to move onward or return home one I’d received medical attention. As it was, I really only experienced that excruciating pain for a couple of hours before getting suitable drugs—that certainly wouldn’t have been the case on the plane. And had I had appendicitis on a US domestic airline, I can’t imagine what would’ve happened or even if anyone would’ve believed me (I certainly don’t have much faith in US domestic airlines). Travel insurance would’ve kicked in (NEVER leave home without travel insurance, particularly if you’re going to the US), but I doubt I’d have been in a fit state to contact the insurance people, and there’s a possibility my luggage wouldn’t have been with me either.
The other scenario is this happening after I arrived in the US. And that’s almost as unthinkable, because I have no idea how I would’ve got treated as a foreigner in another country where all my usual medical safety nets didn’t exist, and where I may have got treated but only after getting the travel insurance to kick it, assuming I was in a mental state to follow that up. How would I have got medical attention and an ambulance anyway? This could’ve happened in a hotel room and I may not have been able to contact anyone to help me (I would’ve been a single traveller). And that’s not considering that I have NO medical insurance (except travel insurance) to cover the costs of the US hospital system, which means that I may not have got treatment in a timely manner and could’ve waited days or weeks for surgery and then be left with an eye-watering bill at the end of it, assuming I survived, or had to pay in full upfront before I got treated.
Which brings me to cost…
Cost of all this
I’ll get a bill for the ambulance (probably about $1000; Update: It was $300 with the 50% rebate applied), but my private health insurance should cover that in full (if I didn’t have private health insurance, I could’ve opted for full ambulance cover for less than $100/year).
I may get some minor bills from the hospital, but that’s unlikely. Most likely, this whole experience (drugs, dressings, IV lines, surgery, doctors, surgeons, nurses, anaesthetists, bed in a public hospital for 2 nights etc.) will cost me absolutely NOTHING. My tax dollars at work!
Why? Because Australia has universal health care for all, which we call Medicare (same name as the US scheme, but a totally different model).
One of my US friends asked how this works, because something like this (or worse), could bankrupt many Americans. So here’s a quick (simplistic) summary of how the Australian health system works:
- Universal health care is a federal responsibility of the Australian Government (states are responsible for providing and staffing public hospitals etc.)
- All Australians who earn above a certain amount (from wages, salary, investments etc.) pay a Medicare levy of between 0 and about 2% on top of their income tax, depending on their taxable income each year. If you don’t earn much, you don’t pay the levy, but you still have access to public hospitals etc. If you earn a lot, you pay around 2% extra on top of your income tax rate, so if you were on the 30% tax rate based on taxable income, you’d actually pay 32%.
- Income tax (and the Medicare levy) is a federal responsibility, so Medicare is for ALL Australian citizens and permanent residents. States raise their taxes in other ways, such as license fees, land tax, etc.
- Public hospitals and some GP visits for some people (such as concession card holders) are funded by our Medicare system, which means we pay nothing for them. BUT for things like elective surgery (knee, hip replacement etc.), the wait lists for such procedures in a public hospital can extend many months and even years, and you won’t get your doctor/specialist of choice, just whoever’s on duty at the time. NOTE: Except in an emergency situation, you cannot see a specialist without going to your GP first and getting a referral—this stops people just calling up a surgeon, for example, and saying they want surgery. Your GP has to assess you first, then refer you to the specialist. The referral letter typically explains their assessment, and in most cases it expires after 12 months, so you have to revisit the GP if you need to see the specialist again at a later date (a real pain for lifelong conditions that need monitoring).
- Emergency department (ED) waits at public hospitals can also be long and as with many EDs around the world you get seen based on medical need (triage), not on your ability to pay. I only know of one ED in a private hospital in my state, though there could be more now—all are in Perth, some 2 hours away.
- Private hospitals also exist, and some specialists and GPs charge well above the set Medicare fee for their services. If you attend any these WITHOUT having private health insurance, or concessions (e.g. pension, veterans card), you would be up for the full cost, which COULD bankrupt you.
- Private health insurance is an option for all Australians, but it NOT compulsory—like any other insurance, you can choose to pay it or not, and how much you pay depends on the level of cover you want. In my case, I’m on top hospital and top ancillary (e.g. dental) cover and I pay about $240/month (just under $3000/year) for that private health insurance. I don’t HAVE to have private insurance… I choose to for the ability to get (elective) surgery done in a hospital of my choosing and with a specialist of my choosing and not be in a very long wait list for similar surgery in the public hospital system. Emergency is a different thing altogether… you need it and need it now. No wait list.
- Depending on your cover, private health insurance may cover you for a stay in a private hospital (often in a private room), specialist attendance while in hospital, some of the gap (co-pay) between the scheduled Medicare fee and what a specialist charges, and other ancillary services, such as dental, optical, physiotherapy etc. Even if I’d had this appendix operation done in a private hospital (most don’t have EDs, so that’s a moot point), it would’ve only cost me $150 co-pay (we call it excess) based on my private health insurance cover plus perhaps some (small) co-pay for anaesthetists etc. Oh, and that $150 excess I’d pay for private hospital surgery? That’s $150 for the year, no matter how many surgical procedures I had to have. Most years I’ve never needed it, but in 2015 I had 3 surgeries (shoulder, eyes, and breast lumpectomy and milk duct removal) and it cost me $150 TOTAL for the 3 hospital procedures, and maybe a bit of co-pay for some of the specialists, but not much (certainly well under $500).
- No health cover in Australia (private or Medicare) is tied to your employer. Employers have NOTHING to do with whether you have coverage or not—the Medicare levy is only based on your income at tax time and the federal government doesn’t care who pays you that income. Private health insurance is your CHOICE and the government doesn’t care about that either. My understanding is that in the US many jobs have the ‘benefit’ of employer-paid health and/or dental insurance—to me, that’s just a very heavy chain to keep you locked in to an employer, never allowing you the freedom to leave that employer, especially if you have sick kids, a disability etc. as you are unlikely to get similar cover with another employer. And god forbid you have your own business or are a freelancer, or are unemployed, or are single and thus have no spouse who has those ‘benefits’ for the whole family!
It would be extremely rare that getting sick in Australia (as an Australian citizen) would come anywhere close to bankrupting you. Our health care system certainly isn’t perfect, but getting sick won’t cost you your home, except in very rare cases. As I said, it’s not perfect, but it sure beats everything I hear about the US system.
Ambulance
In Western Australia, the ambulance system is run by St John Ambulance (SJWA) (other states have different systems). I believe the state government subsidises ambulance costs (50%?) for those meeting certain criteria. In my case, my private health insurance will cover whatever isn’t already covered or subsidised and I should effectively pay nothing.
In regional areas, especially smaller towns, SJWA is purely a volunteer organisation, staffed by angels called community members. I emailed the subcentre that looked after me to thank them for their care, and I got this reply:
Thank you for your delightful email. You made my day and I’m sure all our volunteer ambulance officers will be just as delighted to read your lovely words, especially Wendy and Rodney. It’s not often we get feedback. I’ve never tried the ‘green whistle’ personally but we’ve all seen the magic it can work.
You are why we choose to volunteer. I can’t imagine what the ambulance service would be like without so many dedicated volunteers adding value to the delivery of an ambulance service in a state as vast as WA. Our subcentre is self-funded—we get no direct funds from SJWA nor the State Government. Our funds come from our capacity to invoice our patients and from fundraising by attending events, both of which are set up by SJWA and the WA Health department. Our subcentre does not pay honoraria or wages to any of our workforce—we are all volunteers. We are about to take delivery of a brand new ambulance from monies the subcentre has raised over many years. We are very excited and looking forward to delivery of the ambulance.
And yes, I’d asked about donating to them specifically, and have now done so.